HEALTH CARE FOR ALL
“The biggest enemy of health in the developing world is poverty.”
—UN Secretary-General Kofi Annan, 2001
Current Problem
800 million to 2.5 billion people lack access to essential health services.
Preferred State/What the World Wants
Access to quality local health care for 100% of humanity
Context
A significant percentage of people in the developing world have virtually no
access to meaningful health care. In addition to the lack of health care providers,
another cause, which illustrates the interconnection of our basic human need
problems, is transportation.[1] When they do exist, many people cannot get to
health care facilities because that health care is located in cities or far away
and there is inadequate transportation.
In 2001, close to 53 million women gave birth with no skilled health care worker
in attendance.[2] One tragic result was that close to 500,000 women died in
childbirth that would not have died if they had access to maternal care.
Public health systems are grossly under funded and often concentrated in cities.
In nearly all the countries of sub-Saharan Africa, there are fewer than eight
doctors per 100,000 people.[3] In the U.S. there are 276 doctors per 100,000
people, and Cuba has an astounding 590 doctors per 100,000, the highest ratio
in the world—demonstrating that even a relatively poor nation can care for its
citizens if resources are directed to that priority.[4] Medicine storage and
distribution systems are nonexistent in many poor rural societies, or are poorly
managed, resulting in significant losses of medicines. The World Bank estimates
that for every $100 spent by African governments on drugs, only $12 worth of
medicines reaches patients.[5]
Globally, the relationship between poverty and poor health is dramatic. In the
poorest, least-developed countries, life expectancy is just 49 years and infant
mortality is 80 per 1,000 live births. In high-income countries, the average
life span is 78 years (63% more) and infant mortality rate is five per 1,000
live births (16 times less).[6]
Many things go into making up adequate health. One more obvious component resides
in the domain of adequate food supplies. For example: Every year the world’s
poorest children are robbed of an estimated 130 million years of healthy life.[7]
This tremendous loss to the world is from premature deaths brought about by being
chronically underweight. Other food and nutrition related health problems include
iron deficiency, which is one of the most prevalent nutrient deficiencies in
the world, affecting an estimated two billion people, and causing almost a million
deaths a year. Vitamin A deficiency is the leading cause of acquired blindness
in children. Iodine deficiency causes mental retardation and brain damage. Severe
zinc deficiency causes short stature, impaired immune function and other disorders
and is a significant cause of respiratory infections, malaria and diarrheal disease.
Another food and nutrition related tie-in with health is the mal-nutrition (bad
nutrition) that leads to being chronically over weight. Obesity is killing about
540,000 men and women a year in North America, and 20 countries of Western Europe.[8]
Somewhat surprisingly, it is also reaching into the poorer parts of the world.
Another health problem that can be partially laid on the doorstep of bad nutrition
is alcohol over consumption. Alcohol deaths are proportionally the highest in
the Americas and Europe. It is estimated to cause, worldwide, 1.8 million deaths
per year, including 20–30 percent of oesophageal cancer, liver disease, epilepsy,
motor vehicle accidents, and homicide and other intentional injuries.
In addition to the food and nutrition related causes described above, the leading
global health risk factors are unsafe water, sanitation and hygiene, infectious
diseases, unsafe sex, high blood pressure, tobacco consumption, and indoor smoke
from solid fuels, Together, these account for more than one-third of all deaths
worldwide.
Here is a more detailed litany of global morbidity[9]: cholesterol causes more
than 4 million premature deaths a year, tobacco almost 5 million (over one million
more than it was in 1990), and blood pressure 7 million. Malaria causes over
1 million deaths per year (with more than 300 million seeking treatment[10]),
HIV/AIDS about 3 million. (Life expectancy at birth in sub-Saharan Africa is
currently estimated at 47 years; without AIDS it is estimated that it would be
around 62 years.) Globally, about 2.9 million deaths are attributable to unsafe
sex, most of these deaths occurring in Africa. About 1.7 million deaths a year
worldwide are attributed to unsafe water, sanitation and hygiene, mainly through
infectious diarrhea. (Nine out of ten such deaths are in children, and virtually
all of the deaths are in developing countries.) Nearly 2 billion people are
infected with tuberculosis worldwide.[11]
Half the world’s population is exposed to indoor air pollution, mainly the result
of burning solid fuels for cooking and heating. Globally, it is estimated to
cause 36 percent of all lower respiratory infections and 22 percent of chronic
obstructive pulmonary disease.
One-third of the world’s population continues to lack regular access to essential
drugs. In the poorest parts of Africa and Asia, this figure rises to over 50
percent.[12]
Leading Infectious Diseases
Leading Killers
Health Care for All Strategy 1: Reorient Primary Health Care Around
Community Health Providers
Primary health care is a highly effective, low-cost, culturally appropriate and
rapid approach to providing quality health care to the largest number of people
in any country.[13] Primary health care emphasizes preventive medicine, childbirth
assistance, first aid, basic drug dispensation, nutrition, clean water, sanitation,
and health education. It addresses the key linkages between poverty and health,
and does so in a way that emphasizes capacity building, equity, and affordability.
The approach can be scaled up quickly and has a proven track record.
At the center of this strategy are Community Health Providers, who, with 6 to
9 months of intensive training, followed by supervision and regular retraining,
can handle 75 percent of all the illnesses, health problems, and health care
needs of an individual and a community.[14] A community health worker can provide
first aid for injuries, immunization, antibiotics and other medications, oral
rehydration therapy, growth monitoring, and nutrition information and supplements
(such as iron, zinc and vitamin A). They can give advice and help with births,
natal care, breast-feeding, weaning, contraception and birth spacing, prevention
of AIDS and common illnesses, solutions for sanitation. and other community health
needs—as well as refer seriously ill patients to the nearest health facility.
Community Health Providers are a tried and proven technique for providing health
care. China, Costa Rica, Cuba, and other countries have used this method to make
dramatic improvements in lowering infant, child, and maternal mortality rates,
as well as raising overall life expectancy and other indicators of health.
A national health-care system of hospitals, clinics, and doctors organized around
a well-trained core of community health providers and local clinics could supply
health care equal to almost any in the world, including that found in highly
developed countries such as the United States.[15]
To meet the health-care needs of everyone in the world currently without health
care would take approximately 1 million community health providers—if the recommended
ratio of one per 200 to 250 families were followed.[16] Lowering this recommended
ratio further—to one health-care worker per 150 families so that each can provide
even better care—would cost about $833 million for training of new community
health providers and retraining of existing health workers to fill this role.[17]
Providing supervision, regular retraining, infrastructure support, basic medical
supplies, and salaries for these 1.6 million additional health-care workers would
cost about $15 billion per year.[18] Because health care systems based on patients
paying a moderate fee have been shown to be more efficient and effective than
non-fee systems, the proposed system would charge modest fees for its services
that would cover 20 percent of its costs, bringing down the annual cost to $12
billion.
The community health providers would be an add-on to the existing health care
systems in areas where there is inadequate health care. The current system of
clinics, doctors and hospitals would be re-organized to provide the needed centralized
medical support for this new system. Current government health expenditures would
fund this part of the system.
Health Care for All Strategy 2: Emphasize Health Care for Children
Contained within, and covered by the costs of the above health-care strategy,
is the provision of health care for children that would eliminate the most severe
health problems facing the children of the world. Making sure all children are
reached with health care is one of the most cost-effective strategies the world
can undertake. Insuring that every child is healthy today vastly reduces expenditures
later—as well as increases social and economic well-being. The bedrock of the
truism that prevention is cheaper than cure is health care, and nowhere is it
more true than in health care for children. There is a wealth of available, inexpensive
and easily delivered cures and treatments for most childhood illnesses. Reaching
the children of the world with these will have profound impacts on not just children,
but on the parents caring for these children, their communities and the economies
of which they are a part.
If the above is a strategic reason for an emphasis on a child centered health
system, the following is a tactical reason. In many parts of the world where
health needs are greatest, birth rates are also the highest. Given that one of
the common denominators of all parents is the desire for their child’s well being,
a child centered health system will gain acceptance quickly. As their mother
brings children to the village or town community center to be monitored and have
their health needs met, the mother will also be in the presence of the health
care worker and her health needs will be met. The child acts as the trust builder
that leads to expanded health care coverage for the entire community.
A relatively modest investment in providing health care for children would eliminate
the most severe health problems facing the children of the world. Deploying a
million-plus community health care providers, as outlined in the strategy above,
would go far to accomplish this goal.
Of the nearly 100 million children in the developing world, close to 25 percent
(over 21 million[19]), need to be immunized against measles tuberculosis, diphtheria,
whooping cough, polio and tetanus. Such an effort would prevent 1.6 million deaths
per year among children under five years of age[20] and cost $1 billion.[21]
Immunizing against measles alone would save over 700,000 lives. The measles vaccine,
which costs 26 cents per dose, has been available since 1963. The vaccine cost
for 21 million children would be $5.5 million.
Providing inexpensive oral rehydration therapy for children with severe diarrhea
would save more than 2 million children under the age of five.
About 40 million pre-school children suffer from vitamin A deficiency. At least
250,000 of these children go blind each year, and 28,000 die.[22] Providing vitamin
A to children who lack it in their diet will prevent this tragic condition, as
well as nearly one in four deaths from measles and diarrhea, in which this deficiency
is implicated. Another inexpensive dietary supplement for children that can reduce
deaths is iron for treating anemia caused by malaria.[23]
An investment of $2.5 billion dollars per year for ten years would cover the
costs of a program that will provide immunization against a variety of diseases
for all the world’s children who don’t currently receive such protection, oral
rehydration therapy for 2 million children each year, low-cost antibiotics to
treat pneumonia, anti-malarial drugs, and vitamin and mineral supplements. Also
included in this program would be the parental education and training needed
to implement it on a wide scale.[24]
Health Care for All Strategy 3: Eliminate Iodine Deficiency
More than 700 million people, more than 10 percent of the world’s population,
were diagnosed with goiter brought on by iodine deficiency during the 1990s.
In addition, iodine deficiency is the world’s leading cause of mental defects.[25]
Three hundred million people suffer lowered mental capacity and intellectual
impairment as a result of missing dietary iodine, and three million suffer
from overt cretinism In all, approximately 3 billion people in the world
are at risk in some way from iodine deficiency.[26] For just $40 million
per year, this problem can be eliminated by adding iodine where it is now
missing to table salt or water.[27]
Health Care for All Strategy 4: Prevent and Control HIV/AIDS
The spread of the AIDS epidemic around the world is one of the most alarming
public health developments in the past twenty-five years. There were over
42 million HIV/AIDS-infected people in the world in 2002.[28] Each day,
some 13,700 additional people are infected, or 5 million each year[29]. More
than 22 million children, women and men have died so far--15 million just
in Africa[30]--and 13.4 million children have lost one or both parents to
the disease.[31]
A program to combat HIV and AIDS would include components for preventing
the spread of the disease, caring for its victims, and research toward its
elimination. An investment of $4 billion per year for the next ten years
in 135 low- and middle-income countries for a massive AIDS prevention campaign
would dramatically reduce the number of new cases. Addressing unsafe sex
practices would be an important part of this: by current estimates, more
than 99 percent of the HIV infections prevalent in Africa in 2001 were attributable
to unsafe sex.[32] A study found that 90 percent of sexually active teenagers
in one African country knew nothing about HIV/AIDS. [33] An educational campaign,
or “social vaccine,” directed to this issue could have a dramatic impact
on the further spread of HIV/AIDS. Other preventive measures, based on a
methodology developed by the London School of Hygiene and Tropical Medicine,
the World Bank, and UNAIDS, include teacher education; marketing and promoting
male and female condoms; treatment of sexually transmitted infections;, screening
for syphilis, HIV, and transfusion blood; counseling; preventing mother-to-child
transmission of HIV; mass media campaigns; and education for injection drug
users.[34]
Another $4 billion per year would be invested in providing care and support
to AIDS patients in the same 135 countries in the developing world. Care
and support activities would include diagnostic HIV testing, palliative care,
treatment and prophylaxis for opportunistic infections, highly active antiretroviral
therapy, lab monitoring, and orphan care and assistance.[35]
An additional $1 billion would be invested in a global AIDS research and
development effort to seek a vaccine to prevent or cure AIDS.
Health Care for All Strategy 5: Prevent and Control Malaria
Every year, more than 1 million people in developing countries die from malaria—simply
because they do not have access to effective treatment. Ninety percent of
these deaths are in sub-Saharan Africa,[36] and most of these are children.[37]
Malaria is both a disease of poverty and a cause of poverty. It is a major
constraint on economic development in the way it lowers productivity ($12
billion per year in lost production in Africa alone[38]), discourages tourism
and investment from both outside and internal sources, and adds large burdens
of health care cost to personal and social expenditures—not to mention its
negative impact on general quality of life.[39]
A principle feature of our campaign against malaria would be to scale up
the existing Rolling Back Malaria (RBM) Program, launched in 1998 as a global
partnership of WHO, UNDP, UNICEF, and the World Bank. This program would
work in conjunction with the AIDS prevention and control effort. It would
set up malaria prevention and treatment protocols throughout the malaria-infested
world. It would make highly effective, low-cost sleeping nets available to
all who needed them, deliver treatment to malaria victims, and work on malaria
control and eradication. (Fifty percent of all malaria deaths can be prevented
through the use of bed nets and other prevention and treatment strategies.[40])
The cost of this program would be $3 billion per year for 20 years. $1 billion
of this total would be spent each year on research and development to find
an effective vaccine against malaria.[41]
Health Care for All Strategy 6: Leverage Successful Campaign Against Polio
The fight against polio, if it is successful, will be the most dramatic success
story in public health since the eradication of smallpox. The worldwide incidence
of polio has decreased from 350,000 cases per year in 1988 to 587 new cases
of polio in 2003, and the number of polio-infected countries from 125 to
seven.[42] This astounding 99 percent reduction is the result of a massive
15-year $3 billion campaign and collaboration led by the WHO, UNICEF, the
Centers for Disease Control, and Rotary International. More than 500 million
children in 93 countries were immunized in 2002 alone. Over 2 billion children
have been reached since the start of the global initiative in 1988.
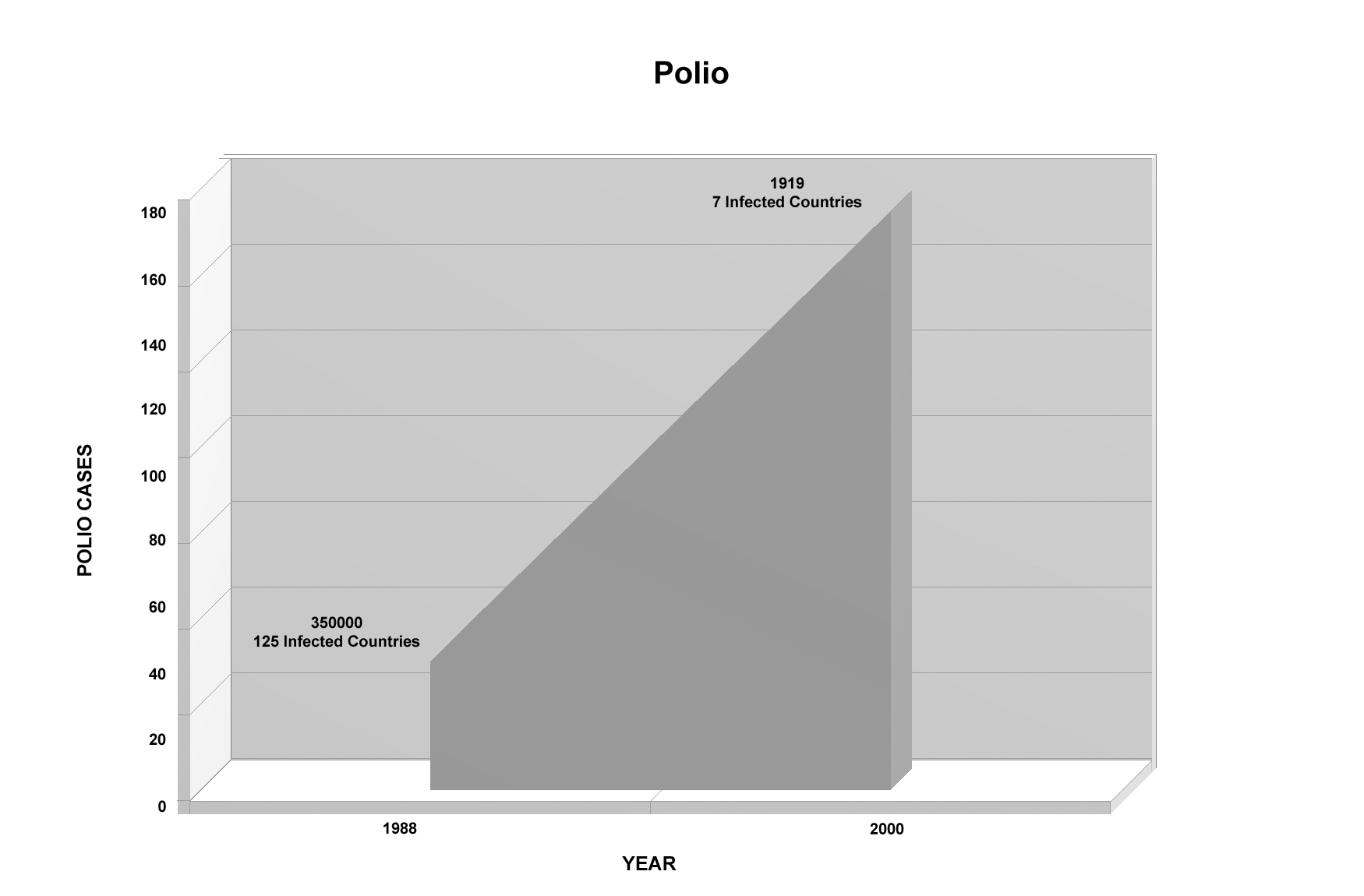
Falling Incidence of Polio
This good news story needs to be finished—and not just in order to finally
eradicate polio so it can join the even more deadly smallpox virus in the
pantheon of vanquished mass killers. There is at least one other very good
reason: it turns out that to get this far toward ending polio required
putting in place an extraordinary infrastructure that has the capacity to
reach children everywhere. This capacity can be (and has already been) used
for other good purposes. For example, over ten million volunteers participated
in mass immunization campaigns in 2002 (some 20 million have been involved
since the beginning of such campaigns [43]. The organizational capacity
needed to pull this off is nothing short of incredible. In just one day in
2000, more than 134 million people in India were immunized against polio.
What else could such an organizational infrastructure be used for? So far,
it has been used for vitamin A distribution. During polio immunization activities
, health workers in 42 countries at the same time administered vitamin A.
Since 1988 over 1.2 million childhood deaths have been prevented through
this action.
This extraordinary global health delivery infrastructure could be used to
carry out other major cross-border health initiatives aimed at reaching large
numbers of people—such as controlling diabetes and hepatitis B; eradicating
guinea worm, measles, and Rubella; eliminating iodine and other nutritional
deficiencies, and ultimately malnutrition itself; and for AIDS education.
To complete the eradication of polio from the world, and to sustain the equally
important volunteer network that has accomplished much of this goal, funding
of $300 million per year for five years would be needed. The already existing
Global Polio Eradication Initiative would be continued and empowered to take
the next steps in working with other scourges of humanity. This initiative
would be incorporated into the Primary Health Care strategy and the other
strategies aimed at providing Health Care for All.
Health Care for All Strategy 7: Reverse the Dangerous Global Rise in Diabetes
Thirty million people had diabetes in 1985. In 1995 the figure was 135 million,
and by 2000 it was 177 million. Although not considered as lethal as AIDS
or malaria, diabetes results in around 4 million deaths per year—more than
from malaria or AIDS-- and it has immense societal and personal costs that
are growing rapidly.
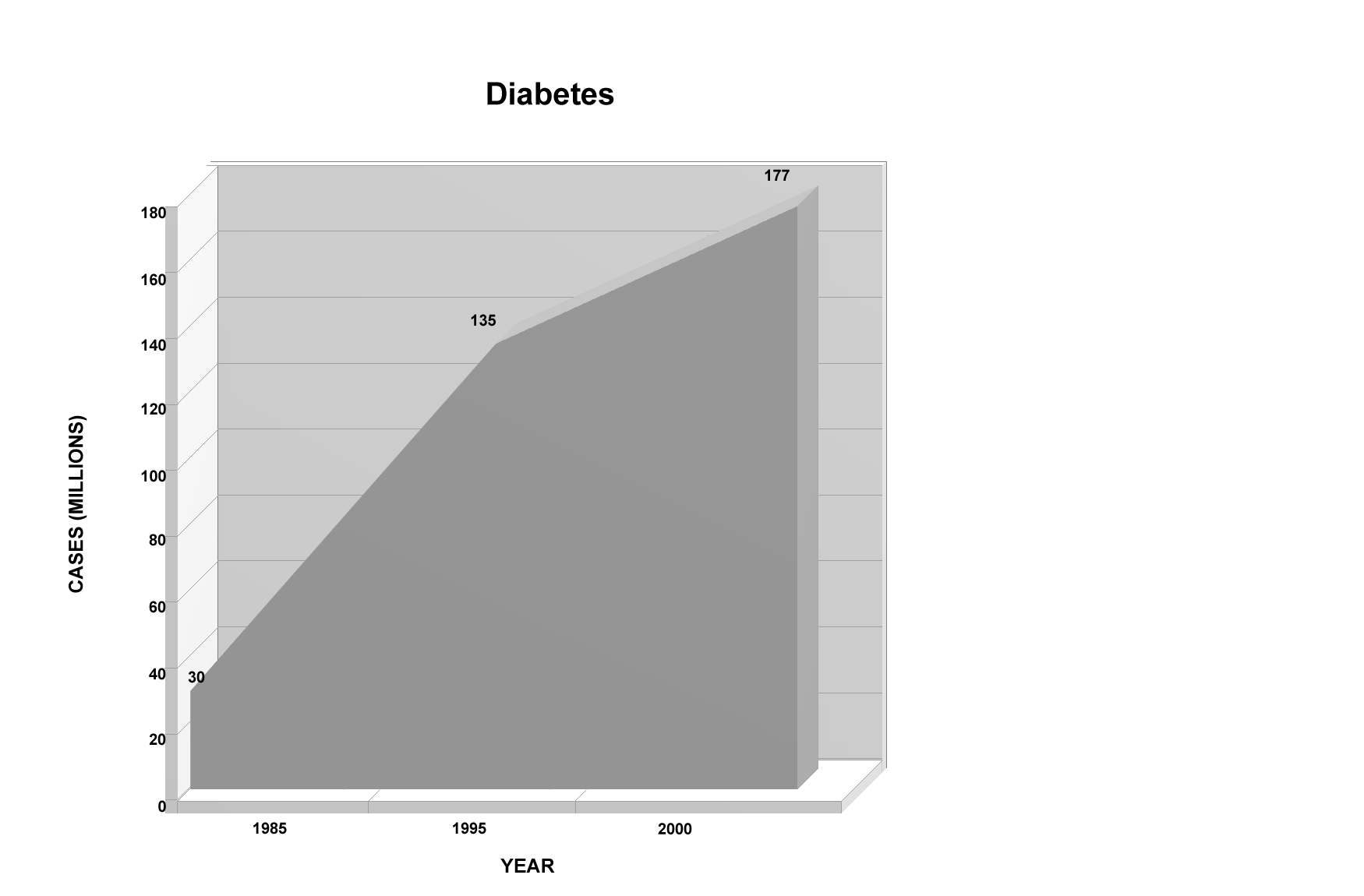
Rising Incidence of Diabetes
For a low-income family in the developing world, the cost of controlling
diabetes in one adult member with the disease can be as much as 25 percent
of family income. In the U.S., the cost is around 10 percent.[44] The total
cost for treating diabetes in the U.S. is $44 billion per year,[45] and this
country’s annual loss in productivity. is $54 billion.[46]
With the benefit of prompt diagnosis and patient education, the massive human
and social costs of diabetes can be sharply reduced. Mass screenings, inexpensive
self-diagnostic technology, and education programs are key components of
a program to control diabetes worldwide. Effective diabetes prevention addresses
other health problems as well: appropriate diet and physical activity lead
to less obesity and cardiovascular disease. A continuous education program
coupled with these actions has reduced diabetes progression by two-thirds
in China, the U.S., and Finland.
The huge costs of diabetes and the equally large payback from a successful
global diabetes reduction program make an expenditure of $1 billion per year
for ten years a low-risk investment.
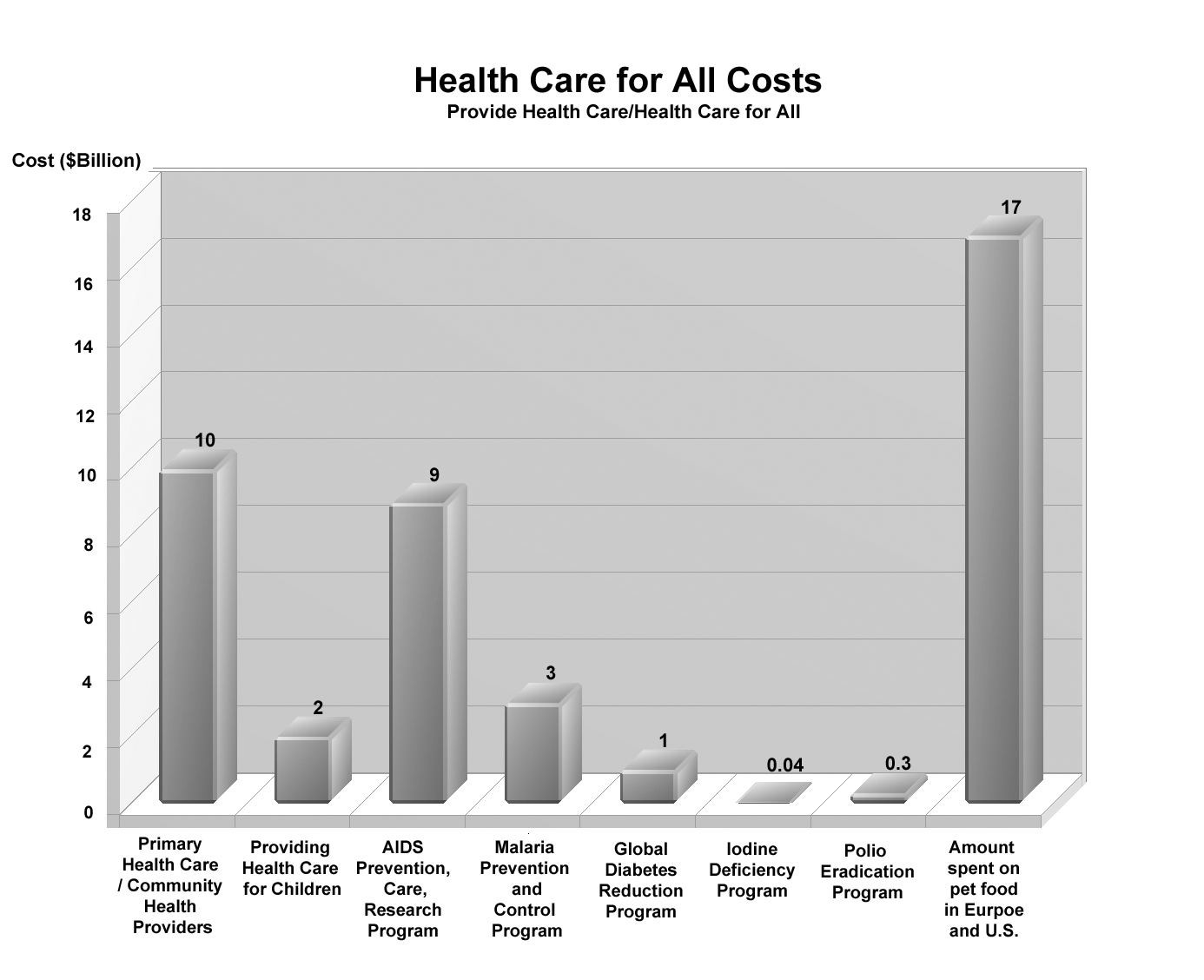
Comparative Costs: Health Care for All
Costs and Benefits—Health Care for All
The total cost of implementing the entire Health Care for All initiative
is $25.34 billion per year for ten years.[47] These funds would be allocated
to the following programs:
* Instituting primary health care systems, which would provide basic health
care to all those who are currently in need, would cost $12 billion per year
for 10 years—equivalent to 1.3 percent of the world’s total annual military
expenditures (less than five days worth), or about 10 percent of what the
United States spends on alcohol each year.[48]
* Providing health care for children would cost $2.5 billion (those funds
included within the budget for Primary Health Care). This is .0032 percent
of the world’s total annual military expenditures—an amount spent on the
military every 28 hours. It is also the amount spent per month on vodka in
the former Soviet Union.[49]
* The $40 million cost of eliminating iodine deficiency from the world is
less than what the U.S. spent in an average four-hour period on the invasion
of Iraq,[50] or .002 percent of what Americans spend on video rentals each
year.
* The $9 billion annual cost for AIDS prevention and control is 24 percent
of what the world spends on hair-care[51], 10 percent of what Europe spends
on alcohol each year, or about .01 percent of the world’s annual military
budget.
* The $3 billion cost of m alaria prevention and control is 15 percent of
what is spent on jewelry worldwide, about 18 percent of what is spent on
controlling illegal drugs in the U.S., or 25 percent of what is spent on
perfume in Europe and U.S. per year.[52]
* The $300 million cost to finish eradicating polio and sustain the valuable
infrastructure from that effort is 2.7 percent of what Europe spends on ice
cream,[53] or 12 percent of what the world military spends each day.
* The $1 billion per year for global diabetes reduction is 12.5 percent of
what the U.S. spends on cosmetics each year.
The combined costs of these programs--$25.34 billion per year for ten years--is
about 63 percent of what the U.S spends on dieting each year. It is also
less than what the U.S. and Japan spend on golf each year[54], or 2.8 percent
of the world’s annual military expenditures, or about what the U.S. and Europe
spend on pet food every 18 months[55], or 19 percent of what the U.S. spends
on alcohol and tobacco per year.[56] Among many possible funding sources
for these health-care strategies, the most productive and life-supporting,,
in terms of increasing human health, would be the subsidies currently given
to health-destroying products that permeate the world’s markets. A 13 percent
tax on cigarettes and alcohol sold in wealthy parts of the world would reduce
the consumption of these substances as well as provide enough funds ($26
billion) to cover the cost of all the global health care programs proposed
here.[57] Legalizing marijuana and taxing its sale could also provide the
needed amounts of revenue.
Another source of funding for health care in the developing world is debt-service
costs. If the debts owed by bankrupt and near-bankrupt countries were “traded”
10 cents on the dollar for payments to enhance education and health care
in these same developing countries, 112 percent of the needed revenue would
be generated.[58] If the most highly indebted poor countries currently eligible
for debt relief used their annual debt service obligations to fund their
health care programs, the entire Health Care for All initiative could be
funded.[59]
Yet another source of funding could be a tax of 1 percent on the gross revenues
of the global pharmaceutical industry. This would bring in more than enough
($3.54 billion) to fund the strategies for children’s health care, ending
iodine deficiency, and supporting the polio campaign.
The benefits of providing adequate health care for everyone in the world
include increased life expectancy, enhanced quality of life, and more productive
working years for hundreds of millions of people. This increased productivity
will lend an economic boost to local societies throughout the developing
world. [60] As a further benefit, the need to provide medical care for diseases
addressed by this initiative will be much reduced.[61] Once polio is eradicated,
the world will save $1.5 billion per year just on vaccination costs. (The
U.S alone spends $250 million per year on polio immunizations.[62] ) Once
eradication is achieved, the reduced need to provide medical care and rehabilitation
for polio victims will mean additional savings—a total of $3 billion per
year.
After all the strategies have been in operation for a decade or more, we
would see comparably huge savings in treatment and related costs for all
the health problems discussed in this chapter. For example, 50 million cases
of tuberculosis can be averted in the next 20 years given the testing, education
and needed drugs according to the World Health Organization.[63]
Another way to quantify the benefits is to look at the value of a human being
in relation to decreased productivity from loss of life and disability. Using
the same values for a human life as in previous chapters, and a formula developed
by the World Bank to calculate productivity lost to disease, the economic
gain to global society from a worldwide health initiative is staggering.
The economic payback for the $21 billion per year investment in these strategies
would be over $10 trillion per year. (See notes for details on this calculation.).[64]
Such an investment pays for itself in less than one day. A better return
on investment is hard to imagine.
Another way of quantifying benefits to the global economy yields even more
astounding results. Begin with the fact that 737 million people in the world
have a life expectancy of less than 50 years.[65] If these people’s life
expectancy were raised to the current average of the world’s high-income
countries (78 years), then 20.6 billion years of productive human life would
be added to the world’s human capital. Assuming a life span of 78 years,
this would be the equivalent of 265 million people. If we valued each of
these lives at $1 million, we add $265 trillion of wealth to the global economy.
Even using a value for each of these lives that is two orders of magnitude
lower—$10,000 apiece—would add $2.6 trillion to the global economy.

Global Life Expectancy
As we have just seen, given adequate food, water, sanitation, and health
care, the wealth of the world skyrockets. Although these advances will have
made us both immeasurably and measurably richer in many areas of life—richer
than we have ever been in history—we are not yet billionaires, or even mere
millionaires. But we’re just getting started.
“Health is not merely the absence of disease or infirmity but a state of
complete physical, mental and social well-being.”
—World Health Organization
“A child born in a developing country runs a 1,000 fold greater chance of
dying from measles than a child born in an industrialized country.”
—World Health Organization
“As long as a single child remains infected with poliovirus, children in
all countries are at risk of contracting the disease.”
—World Health Organization
------------------------------------------------------------------------
[1] Pharmaceutical Research and Manufacturers of America, Health Care in
the Developing World, http://world.phrma.org/healthcare.devel.world.html
[2] UNDP, Human Development Report 2003 (New York, UNDP 2003, p. 257). The
% of births attended by skilled health personnel was 60; total births is
136 million.
[3] UNDP, Human Development Report 2003 (New York, UNDP 2003, p. 256). South
Africa is the exception. It has 443 doctors per 100,000 people, 60% more
than the U.S..
[4] UNDP, Human Development Report 2003 (New York, UNDP 2003, p. 255). China
has 167 per100,000 and India 48.
[5] Pharmaceutical Research and Manufacturers of America, Health Care in
the Developing World, http://world.phrma.org/healthcare.devel.world.html
[6] UNDP, Human Development Report 2003 (New York, UNDP 2003, p. 212 for
infant mortality and p. 240 for life expectancy).
[7] WHO, The World Health Report 2002, http://www.who.int/whr/en/
[8] WHO, The World Health Report 2002
[9] ibid. Unless otherwise noted.
[10] Victoria McGovern, Queta Bond, “Global Health Research” (Science, June
27, 2003, p. 2003).
[11] ibid.
[12] WHO, Globalization and Access to Drugs
[13] UNICEF, State of the World’s Children 1996, p. 39.
[14] UNICEF, State of the World’s Children 1996, p. 41.
[15] Costa Rica has raised life expectancy to 76.1 years, just a little less
than that of the U.S. rate of 77. Cuba’s life expectancy is 76.9. A community
health worker sees each child in Costa Rica at least once per month, more
than the average child sees a health worker in the U.S.
[16] UNICEF, State of the World’s Children 1990 (New York: Oxford University
Press, 1990). p. 41. Assuming a conservative 4 people per family,
[17] Derivation based on UNICEF, State of the World’s Children 1990, p. 41.
If one health care worker is needed for every 250 families, then one million
are needed to meet the needs of one billion people. If one health care worker
is needed for every 150 families, then 1.6 million health care workers are
needed. At the average training cost of $500 per worker (UNICEF, p. 41),
total training would cost $833 million.
[18] $8.8 billion per year for salaries, $5.2 billion for supervision, retraining
and infrastructure. Salary scale derived from UNICEF, State of the World’s
Children 1990, pp. 41-43. Applying a salary of $5,500 to each of 1.6 billion
health care workers gives a total of $8.8 billion.
[19] UNDP, Human Development Report 2003, (New York, UNDP 2003, p. 257)..
[20] WHO, Removing Obstacles to Healthy Development (Geneva, WHO, 1999).
[21] “Urgent call to improve survival of millions,” (WHO, June 23, 2003)
www.who.int/mediacentre/releases/2003/pr52/en/print,html
[22] WHO, The World Health Report 2002 Annex Table 2 Deaths by cause, p.
186
[23] Ibid. p. 17.
[24] UNICEF, State of the World’s Children 1990, p.16.
[25] C. K. Pralahad, The Fortune at the Bottom of the Pyramid, (Philadelphia,
Wharton School Publishing, 2004, p. 173).
[26] International Council for the Control of Iodine Deficiency Disorders
(ICCIDD) http://www.people.virginia.edu/~jtd/iccidd/mi/regions/world_summary.htm
(1-05).
[27] UNICEF, State of the World’s Children 1990, p. 36. Based on 5¢ per person/year.
[28] United Nations Programme on HIV/AIDS (UNAIDS) AIDS Epidemic Update:
December 2002 (Geneva, 2002, p 3.)
[29] ibid.
[30] “Slowly the virus is being fought,” (The Economist, September 27, 2003,
p.45).
[31] UNFPA, State of the World Population 2002: People, Poverty, Possibilities:
Making Development Work for the Poor. (New York, United Nations Population
Fund, 2003).
[32] Pharmaceutical Research and Manufacturers of America, Health Care in
the Developing World, http://world.phrma.org/healthcare.devel.world.html
[33] UNFPA, State of the World Population 2002: People, Poverty, Possibilities:
Making Development Work for the Poor. (New York, United Nations Population
Fund, 2003).
[34] B. Schwartlander, et. al., “Resource Needs for HIV/AIDS,” (Science,
June 29, 2001, p. 2434).
[35] Ibid. p. 2435.
[36] Louis H. Miller, Brian Greenwood, “Malaria—A Shadow over Africa,” Science,
October 4, 2002, (Washington DC, 2002)
[37] “Clearing the air,” (The Economist, September 27, 2003, p. 82).
[38] Ibid. Also: WHO, Removing Obstacles to Healthy Development (Geneva,
WHO, 1999, p. 32) estimates $500 million direct costs per year in Sub-Saharan
Africa alone.
[39] WHO, Roll Back Malaria Fact Sheet, #10 “Economic costs of malaria” (Geneva,
March 2002) www.rbm.who.int
[40] WHO, Removing Obstacles to Healthy Development (Geneva, WHO, 1999, p.
15).
[41] Jeffrey D. Sachs, “A New Global Effort to Control Malaria” Science,
October 4, 2002, p. 129. (Washington DC, 2002)
[42]UNESCO, India launches largest ever campaign to tackle polio epidemic,
(Paris, UNESCO, 2003). http://www.unicef.org/newsline/2003/03pr05polio.htm
[43] Rotary International: http://www.rotary.org/newsroom/presscenter/releases/182.html
[44] WHO, “The Cost of Diabetes” Fact Sheet 236, September, 2002
[45] Yearly cots in Brazil are estimated at $3.9 billion, Argentina at .8
billion, Mexico at $2 billion. Each of these costs is rising. Over all the
direct health care costs of diabetes range between 2.5% to 15% of annual
health care budgets. ibid.
[46] ibid.
[47] and $4 billion for another ten years for a total of 20 yers for malaria
control.
[48] U.S. spent $116 billion on alcohol in 2002; (Bureau of Economic Analysis,
Department of Commerce).
[49] UNICEF, State of the World’s Children 1990, p.16.
[50] National Priorities. www.nationalpriorities.org/issues/ military/iraq/MAcities.html
Various groups, including National Priorities, have estimated the cost of
the Iraq war at $100 billion.
[51] “Fast-growing business,” (The Economist, May 26, 2001, p. 68).
[52] UNDP Human Development Report 1998, www.undp.org
[53] UNDP Human Development Report 2002, www.undp.org
[54] U.S. golf expenditures: $24 billion; Japan, $$3.1 billion; U.K. 1.5
billion
[55] Pet food costs: Ann Pettifor, Jubilee 2000, Debt Relief and MDG’s www.jubileeresearch.org;
Europe and the U.S. spend $17 billion/year or $1.416/month on pet food.
[56] U.S. spent $131.95 billion on alcohol and tobacco in 1995; (Bureau of
Economic Analysis, Department of Commerce).
[57] Alcohol and tobacco consumption in Europe, Japan and North America is
well in excess of $200 billion/year.
[58] Total developing country debt is $2.4 trillion; high debt poor countries
have more than $283 billion in debt. 10% of the lower figure is $28.3 billion.
[59] Assuming a 10% interest rate and $283 billion total debt.
[60] African economies have lost approximately $100 billion over the past
35 years due to malaria alone. (Worldwatch Institute, Vital Signs 2001, www.worldwatch.org)
They also lose 1% per year in economic growth (J. Sachs et al., Nature 415,
680; 2002)
[61] Malaria may account for as much as 40% of public health expenditure,
30-50% of inpatient admissions and up to 50% of outpatient visits in areas
where malaria is a heavy burden.
[62] WHO, Removing Obstacles to Healthy Development (Geneva, WHO, 1999, p.
22).
[63] “Gambling with lives,” (The Economist, June 2, 2001, p. 14).
[64] Figured in the same way that the previous strategies for eliminating
starvation related deaths. Each life saved being “worth” $1 million and 10
million lives saved per year as a result of global health care coverage.
The World Bank measures the loss in human productivity due to disease in
“disability-adjusted life years,” or DALYs. There have been 1.36 billion
disability-adjusted life years lost each year since 1990. Using this as a
measuring stick, and assuming that 70 of these “life years” adds up to one
life, and valuing each of these lives (19.43 million lives) at $1 million
results in $19.43 trillion or about 40% of the Gross World Product. Valuing
each life an order of magnitude lower, at $100,000, results in $1.94 trillion
per year. A more modest payback to the global economy was figured by the
WHO’s Commission on Macroeconomics and Health which figured the economic
gain for a similar investment at $186 billion peryear, or about $23,250 per
life saved (in The Economist, “The health of nations,” December 22, 2001,
2001, p. 83).
[65] UNDP, Human Development Report 2003, (New York, UNDP 2003, p. 240).
[66] WHO, Removing Obstacles to Healthy Development (Geneva, WHO, 1999).
[67] Carter Center, January 26, 2004
[68] WHO, The World Health Report 2002 Annex Table 2 Deaths by cause, p.
186.
[69] Howard Markel, “The Epidemic Scorecard,” (The New York Times, 4-30-2003,
p. A27).
Back to Price of Peace